

Art Attacks: Biological Affect of Beauty
Stendhal Syndrome, a rare psychosome condition where an individual experiences acute physical and mental symptoms when exposed to overwhelming beauty

Stendhal Syndrome, a rare psychosome condition where an individual experiences acute physical and mental symptoms when exposed to overwhelming beauty, occupies a striking intersection of neuroaesthetics, psychophysiology, and embodied cognition. The condition raises fundamental questions about the biological basis of aesthetic experience - specifically, the extent to which culturally charged perceptual encounters can produce measurable physical symptoms.
Marie-Henri Beyle - better known by his pen name Stendhal - described his visit to Florence and Santa Croce in Rome, Naples et Florence (1817) as a deeply physiological experience prompted by an overwhelming aesthetic encounter: “Absorbed in the contemplation of sublime beauty ... I reached the point where one encounters celestial sensations ... Everything spoke so vividly to my soul. Ah, if I could only forget. I had palpitations of the heart, what in Berlin they call ‘nerves’. Life was drained from me. I walked with the fear of falling.”

What Stendhal described that January day has since lent its name to one of the more unusual conditions in the literature of psychosomatic medicine. Stendhal Syndrome - also known as Florence Syndrome or hyperkulturemia - refers to an acute physical and psychological response triggered by exposure to works of great beauty, typically concentrated in a single space such as a museum (Magherini, 1989). Its symptoms range from tachycardia and dizziness to dissociation, paranoia, and, in rarer cases, hallucinations. Dario Argento visualises the symptoms in the thriller movie The Stendhal Syndrome, in which the main character Anna becomes overwhelmed upon experiencing art.
It was not until the late 1970s that the phenomenon was systematically studied. Graziella Magherini, then chief of psychiatry at Florence’s Santa Maria Nuova Hospital, began noticing a consistent pattern: tourists admitted to her ward were not simply suffering from exhaustion or heat, but something their own accounts described as “a painful and numbing ecstasy”. Between 1977 and 1986, she recorded 106 such cases, all among foreign visitors to Florence (Magherini, 1989). She organised the cases into three clinical categories: predominantly psychotic presentations such as paranoia and perceptual disturbances (the majority), affective disturbances including episodes of euphoria or depression, and anxiety with physical symptoms expressed through panic and chest pain. She named the condition after Stendhal.
What is striking about these cases is not the occurrence itself but their specificity. Patients did not collapse from general tourist fatigue - they collapsed in front of particular objects. One of the patients, a man named Franz, developed intense tachycardia before Caravaggio’s Adolescent Bacchus. A visitor named Lilibet, standing before Donatello’s David in the Bargello, felt the sculpture looking back at her - felt it begin to fall upon her - and believed she was losing her mind (Magherini, 1989). And while it could be argued that these are extreme outliers, they open up a valuable dialogue about the way we physically experience art and aesthetic encounters.

Despite Magherini’s decade of clinical work, Stendhal Syndrome has never been formally recognised by the DSM or the ICD, and skepticism has followed it throughout its history. Critics have proposed that the cases represent little more than travel exhaustion compounded by ambient heat, or the product of a romantic cultural expectation that Florence ought to overwhelm the visitor - a self-fulfilling psychological prophecy (Bamforth, 2010; Innocenti et al., 2014).
While these critiques have force, they struggle to account for the clinical consistency of Magherini’s case series, and they say nothing about what happens, physiologically, when a human being stands before an image of exceptional aesthetic and cultural power. That question has become, in recent decades, the domain of neuroscience.
Research in neuroaesthetics has established that viewing art is far from a passive act - it actively recruits the brain’s sensorimotor systems through a process known as embodied simulation, in which the brain responds to depicted bodies and forms as if they were physically present (Gallese, 2009). Vittorio Gallese’s work on mirror neurons suggests that when we look at a painted figure, we are, at a neural level, inhabiting it: internally rehearsing its posture, its implied motion, and its emotional state.
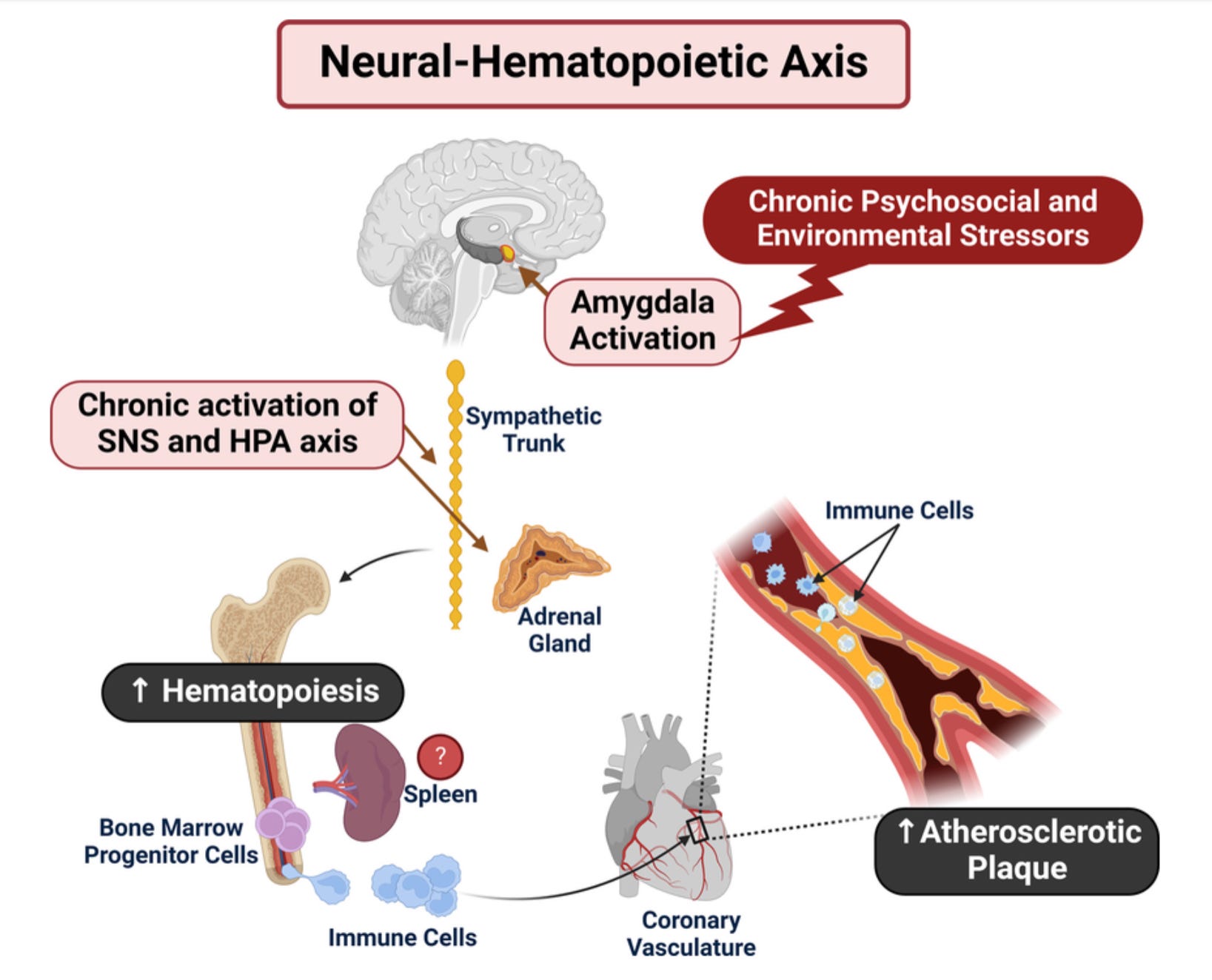
Studies on the coupling between bodily sensation and aesthetic response have found that heart rate can accelerate or shift in response to both music and visual stimuli, pointing to a deep connection between what we perceive in the world and our internal physical state (Azevedo & Tsakiris, 2017). More directly relevant to the Uffizi cases is research by Tawakol et al. (2017), published in The Lancet, which identified what the authors termed a “neural-hematopoietic axis” - a biological pathway linking activity in the amygdala (the brain’s threat and emotion centre) to cardiovascular events via downstream effects on bone marrow and arterial inflammation. Higher amygdala activation, they found, correlates with elevated cardiovascular risk. Separately, research on the amygdala’s response to imagery has shown that this structure is activated not only by threatening stimuli, but also by images of significance or beauty that violate prior expectations (Ewbank et al., 2009).
Drawing these findings together in the context of the museum experience, a clearer picture begins to emerge of what may have occurred in Magherini’s patients. A viewer with heightened aesthetic sensitivity, surrounded by a dense concentration of masterworks and engaged in embodied simulation of emotionally charged figures, may be sustaining elevated amygdala activation - with downstream cardiovascular effects that, in individuals with particular physiological vulnerabilities, could place real strain on the heart. This is, in effect, what we might call an “art attack”.
The broader phenomenon described by Stendhal Syndrome appears to recur across cultures and historical periods under different names. The so-called Paris and Jerusalem Syndromes document similarly acute physical and psychological responses triggered by aesthetic or spiritual encounters. Paris Syndrome, a term introduced in the 1980s by Japanese psychiatrist Hiroaki Ota, is characterised as a crisis of shattered cultural expectation: visitors whose image of Paris has been shaped by cinema and high fashion can experience a jarring collision with the ordinary reality of a modern city, leading to reported symptoms including hallucinations, depersonalisation, heart palpitations, dizziness, and rapid heart rate. Jerusalem Syndrome, by contrast, involves an intense religious identification or delusion triggered by the city’s spiritual associations, in some cases producing psychotic episodes such as the belief that one is a reincarnation of a biblical figure.

It would be easy to read Stendhal Syndrome as evidence of art’s danger, or as a curiosity confined to unusually sensitive individuals. But the accumulating body of evidence surrounding this and related phenomena has real value when considering the depth of the human aesthetic response - the fact that beauty is something the body registers as urgent, as real, and as physiologically significant.
Art historians have long observed that the boundary between aesthetic experience and physical response is a permeable one. Bernard Berenson described the “aesthetic moment” as a state in which the observer and the artwork dissolve into one another - time abolished, selfhood suspended (Berenson, 1948). Proust reportedly experienced dizziness and near-loss of consciousness before Vermeer’s View of Delft. Dostoyevsky was reportedly left motionless before Holbein’s Dead Christ. These are not the reactions of fragile people to overwhelming stimuli. They are extreme expressions of something universal: the capacity of art to break through the constraints of its medium and produce responses that are entirely, undeniably physical.

Stendhal himself, recovering on the steps of Santa Croce, ultimately concluded that the episode had been worth it. He wrote two days later that the memory of what he had felt gave him a kind of pride - that it was better to have a sensibility capable of such response than any social distinction (Stendhal, 1817). The syndrome, in his own reckoning, was not an illness, but rather, a life-affirming experience.
Aesthetic experience activates the brain’s reward circuitry, modulates the body’s internal state, and engages the amygdala in ways that blur the line between merely seeing and genuinely feeling. That this can occasionally go further than expected - that the connection between art and body sometimes carries more weight than we anticipate - is not a warning against engaging with art. It is a reason to take seriously the place that art occupies in our understanding of human biology and behaviour.
Azevedo, R. T., & Tsakiris, M. (2017). Art reception as an interoceptive embodied predictive experience. Behavioral and Brain Sciences, 40, 17–18.
Bamforth, I. (2010). Stendhal’s syndrome. British Journal of General Practice, 60(581), 945–946.
Barnes, J. (2008). Nothing to be frightened of. Random House Canada.
Berenson, B. (1948). Aesthetics and history in the visual arts. Pantheon.
Ewbank, M. P., Lawrence, A. D., Passamonti, L., Keane, J., Peers, P. V., & Calder, A. J. (2009). The amygdala response to images with impact. Social Cognitive and Affective Neuroscience, 4(2), 127–133.
Gallese, V. (2009). Mirror neurons, embodied simulation, and the neural basis of social identification. Psychoanalytic Dialogues, 19(5), 519–536.
Innocenti, A., D’Ambrogio, T., & Castellini, G. (2014). The Stendhal Syndrome between psychoanalysis and neuroscience. Rivista di Psichiatria, 49(2), 61–66.
Magherini, G. (1989). La sindrome di Stendhal. GEP spa.
Takaes de Oliveira, I. (2020). One touch of Venus: Notes on a cardiac arrest at the Uffizi. Figura: Studies on the Classical Tradition, 8(1), 115–149.
Tawakol, A., Ishai, A., Takx, R. A. P., Figueroa, A. L., Ali, A., Kaiser, Y., … Pitman, R. K. (2017). Relation between resting amygdalar activity and cardiovascular events: A longitudinal and cohort study. The Lancet, 389, 834–845.
Stendhal [Marie-Henri Beyle]. (1854). Rome, Naples et Florence. Michel Levy Ed. (Original work published 1817)